
Key Takeaways
- Four upstream decisions drive most disparities you can influence: how mood versus psychotic features are weighted, mood stabilizer use in suspected bipolar, how adherence is interpreted, and which therapy partners receive referrals.
- When Black or Hispanic patients present with mixed features, build the mood differential first and document quantitative scores like PHQ-9 or YMRS before psychotic symptoms become the organizing diagnosis 9.
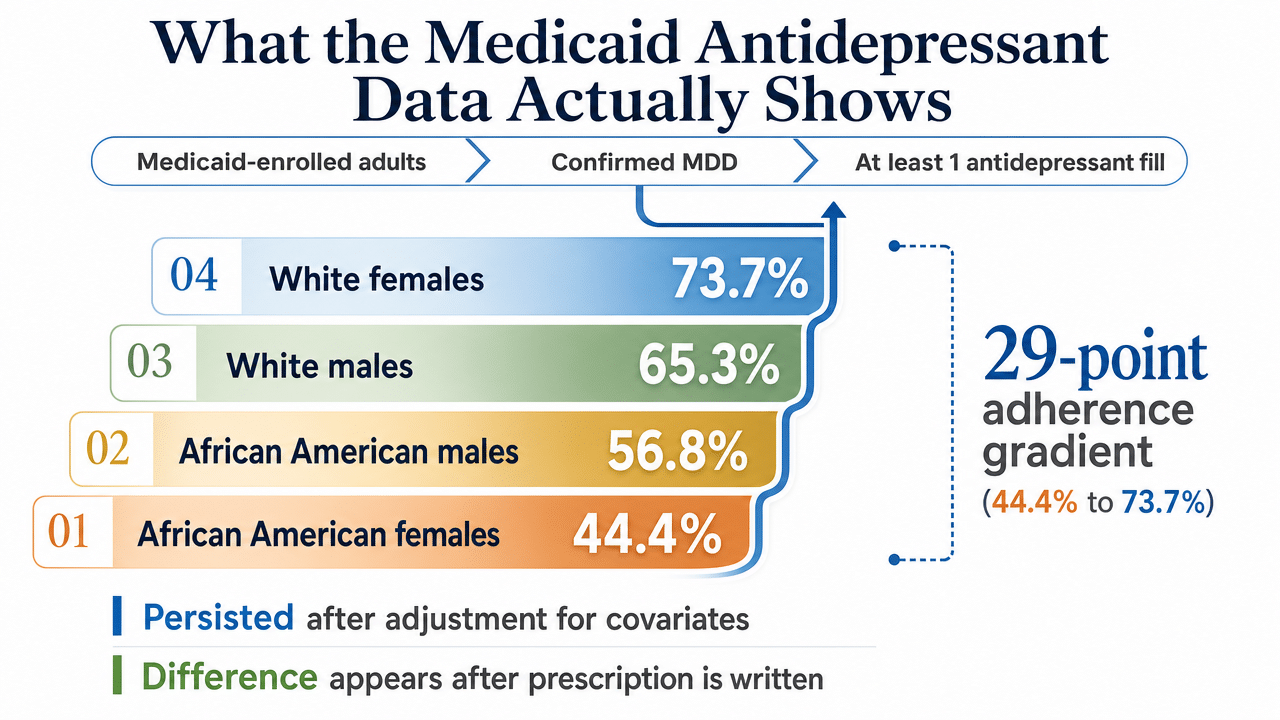
- Read low adherence as diagnostic data about the encounter, not a patient trait — Medicaid antidepressant adherence ran 44.4% in Black women versus 73.7% in white women after covariate adjustment 12.
- Start with a ten-chart self-audit covering mood documentation, mood stabilizer presence under schizophrenia labels, two-week follow-up cadence after SSRI starts, and specificity in adherence notes to surface your own drift points 1.
Where Disparities Actually Enter Your Clinical Workflow
If you’ve been practicing psychiatry or working as a PMHNP for any length of time, you already know the disparities literature exists. You’ve seen the headlines, sat through the trainings, maybe even rolled your eyes at a slide deck that defined cultural competence in three bullet points. That’s not what this article is about.
What’s worth your time is something narrower and more useful: the specific points in your clinical workflow where documented disparities actually show up and change what you prescribe. Not as a values discussion, but as a diagnostic and treatment-planning question. Prevalence of most psychiatric disorders is similar or lower in racial and ethnic minority populations compared with white populations, yet treatment quality is consistently worse 1, 10. That gap isn’t closed by good intentions. It’s closed by tightening four decisions that sit upstream of outcomes.
Those decisions are: how you weight mood versus psychotic symptoms in your differential, which medication class you reach for in suspected bipolar presentations, how you interpret a missed refill or a flat PHQ-9 response, and how you choose the therapy partners you refer to. Each one is a place where the data shows a measurable skew, and each one is something you can adjust on Monday morning without restructuring your practice.
The sections that follow walk through the evidence at each touchpoint and what to do with it. The goal isn’t to make you feel worse about a hard job. It’s to give you sharper handles on the parts of the encounter you actually control.
The Diagnostic Asymmetry Problem
Mood Symptoms Get Underweighted in Black Patients Presenting With Psychotic Features
Here’s the finding that should change how you sit with a mixed presentation: among African American patients admitted for psychiatric care, the rate of schizophrenia diagnosis runs roughly five times higher than among white patients 8. That multiplier is drawn from a literature review of empirical studies in U.S. inpatient and forensic settings, not a general outpatient sample, so apply it where it fits. But the mechanism it points to travels with you into every clinic room.
The Rutgers study that examined more than 1,600 patients with severe depression found that clinicians were more likely to emphasize psychotic symptoms over depressive symptoms in African American patients, even when mood symptom severity was comparable across racial groups 9. That’s the part worth sitting with. The patients weren’t presenting differently. The clinicians were weighting differently.
You probably don’t experience this as bias in the moment. It feels like clinical judgment. A patient describes paranoia about a landlord, or reports hearing a deceased grandmother’s voice during a grief episode, and the salience of those details rises in your assessment. The mood content, especially when it’s expressed as somatic complaints, irritability, or guarded affect, recedes. The diagnosis that emerges fits what you noticed, not necessarily what was there.
The downstream cost is significant. A patient labeled with a primary psychotic disorder gets antipsychotics first, often without an adequate trial of antidepressants or mood stabilizers, and carries that chart label forward for years. Subsequent prescribers anchor on it. The original diagnostic asymmetry compounds into a treatment trajectory that’s hard to reverse, particularly if the patient stops engaging because the medications don’t match what they’re actually experiencing.
You can’t fix the literature, but you can change what you do with an ambiguous presentation in front of you.
Bipolar Misclassification and the Mood Stabilizer Gap
The same diagnostic skew shows up one shelf over, in bipolar disorder. Patients of African ancestry with bipolar disorder are more often misdiagnosed with a different condition, frequently schizophrenia, and are less likely to receive mood stabilizers than patients of non-African ancestry 11. Hispanic patients show similar patterns of misclassification and suboptimal treatment.
Think about what that means at the prescription pad. A patient who actually has bipolar I, presenting in a mixed or psychotic mania, gets read as primary psychosis. You write for an antipsychotic. The acute episode resolves, partially. The mood instability underneath doesn’t. Without lithium, valproate, or lamotrigine in the regimen, you’re managing a chronic illness with the wrong long-term tool. Cycling continues. The patient comes back, and the chart still says schizophrenia.
There’s a second-order problem the review flags directly: minority groups remain underrepresented in bipolar disorder clinical trials 11. That means the efficacy and tolerability data you rely on for medication selection were generated in samples that don’t fully reflect the patient sitting across from you. You’re not wrong to use the evidence base. You should know its edges.
What this changes in your prescribing: when you see psychotic features in a Black or Hispanic patient who also has a credible mood history, take the mood history seriously enough to consider a mood stabilizer trial, not just an antipsychotic. A family history of bipolar or depression, prior antidepressant-induced activation, periods of decreased need for sleep with goal-directed activity, postpartum episodes in female patients with depressive presentations — these are the data points that often get under-collected because the visit anchored on what was acute, not what was longitudinal. Slowing down on the history before reaching for the prescription pad costs you maybe ten minutes. It can change a decade of care.
Practical Adjustments to Your Differential
None of this requires you to second-guess every diagnosis you make. It requires a few small habits at the points where the literature says you’re most likely to drift.
When a Black or Hispanic patient presents with both mood and psychotic features, build the mood differential first, then ask whether the psychotic features fit better as mood-congruent, mood-incongruent within an affective episode, or as a primary thought disorder. The order matters. Building the schizophrenia differential first and then asking whether mood fits inside it is how you end up underweighting the depression 9. Reversing the sequence forces the depressive and manic criteria to get a full hearing before psychotic symptoms become the organizing principle.
Document mood symptom severity quantitatively. A PHQ-9 or YMRS score in the chart at intake creates an anchor you and any subsequent clinician can return to. Without it, mood data tends to be summarized in adjectives that fade against the more specific language of psychotic symptoms.
When you inherit a schizophrenia diagnosis on a Black or Hispanic patient and the longitudinal course doesn’t fit — episodic rather than continuous, clear interepisode functioning, prominent mood features in the history — treat that chart label as a hypothesis, not a fact. Ask the patient directly about mood episodes, family psychiatric history, and what their first episode looked like. The Institute of Medicine review names this kind of systematic incorporation of sociocultural and longitudinal information into reassessment as a provider-level lever you can actually pull 1.
This is hard work, especially in a fifteen-minute med check. The data is uncomfortable. Small shifts in your differential, applied consistently across the patients where the literature says you’re most likely to drift, are how the gap closes one chart at a time.
Reading Adherence as a Signal, Not a Trait
What the Medicaid Antidepressant Data Actually Shows
Here are the numbers that should reframe how you read a missed refill. Among Medicaid-enrolled adults with major depressive disorder, antidepressant adherence rates broke down like this:
- African American females at 44.4%
- African American males at 56.8%
- white males at 65.3%
- white females at 73.7% 12
The gradient persisted after adjustment for covariates, which means socioeconomic status alone doesn’t explain it. Something else is moving.
Read those numbers carefully before you reach for an interpretation. The study population is Medicaid enrollees with a confirmed MDD diagnosis who filled at least one antidepressant prescription. So the cohort already cleared two filters: diagnosis and initial fill. The disparity you’re seeing is what happens after the prescription is written, not whether it gets written. That distinction matters because it locates the problem in the longitudinal arc of treatment, not in initial access.
The temptation, especially under time pressure, is to fold this into a story about patient-level factors. Health literacy. Side effect tolerance. Beliefs about medication. Those factors are real and worth asking about. But when a 29-point adherence gap separates two groups of patients carrying the same diagnosis in the same payer system, the explanation that fits is structural and relational, not individual. The authors of the study point directly to socioeconomic factors, trust, and care fragmentation as the likely drivers 12.
When Nonadherence Is Telling You About the Encounter
Adherence in psychiatric medication is rarely a single decision. It’s an accumulating series of small ones: take it this morning, skip it because of the headache, restart Monday, run out before the refill, decide it wasn’t doing much anyway. By the time it shows up in your data as a 60-day gap, the patient has made dozens of micro-decisions you weren’t in the room for.
What the literature suggests is that those micro-decisions track with how the patient experiences the prescriber. Minority patients with depression are more likely to report lower perceived cultural understanding from their clinicians, and that perception correlates with engagement 3. When a patient doesn’t feel heard about what the medication is actually doing in their body and life, the next dose becomes optional in a way it isn’t when they feel like a partner in the plan.
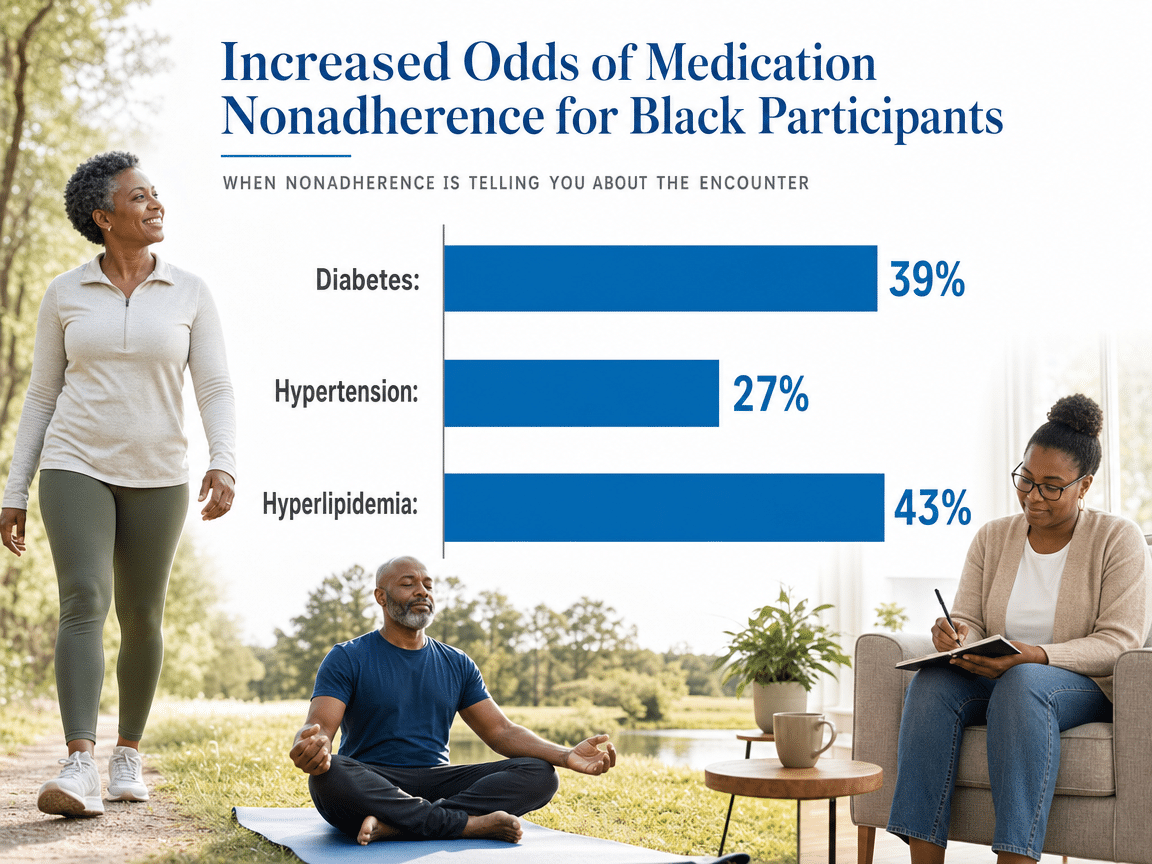
This pattern isn’t limited to psychiatry. A Medicare medication therapy management study found Black participants had 39%, 27%, and 43% higher odds of nonadherence to diabetes, hypertension, and hyperlipidemia medications, respectively, compared with white participants 2. The same relational and structural dynamics show up across conditions. What’s different in psychiatry is that the medication itself is harder to feel working in the first three to six weeks, and the side effects often arrive before the benefits.
So when you see a Black or Hispanic patient with poor adherence on an SSRI, treat it as a prompt to ask a specific set of questions. What is the medication doing that you didn’t expect? What did you think it would do that it’s not doing? Is there something about taking it daily that doesn’t fit your life right now? Those questions surface side effects you didn’t hear about at the last visit, beliefs about the medication you didn’t get to address, and dosing problems you can actually solve. The data tells you where to look. The conversation tells you what to change.
Follow-Up Cadence as a Clinical Lever
One of the most underused tools you have for adherence is also the simplest: when the next visit is scheduled. Standard initial follow-up after an SSRI start is often four to six weeks, which assumes the patient will navigate the first month — including the period when side effects peak and benefits haven’t arrived — without much contact.
For patients where the literature flags elevated risk of early discontinuation, that cadence is probably wrong. Pulling the first follow-up in to two weeks, even as a brief telehealth check, changes what’s possible. You catch side effects before they become reasons to stop. You hear how the patient is actually experiencing the medication while there’s still time to switch or adjust. You signal that the relationship continues past the prescription.
This is not about flagging patients by race and creating a parallel schedule. It’s about recognizing that your default cadence was calibrated for a patient profile that doesn’t match every patient in front of you. The Institute of Medicine review identifies systematic incorporation of sociocultural and longitudinal information into care planning as a provider-level lever that maps to better outcomes 1. Visit frequency is one of the clearest places that lever lives.
If your practice can’t accommodate two-week visits across the board, a phone or portal-based check-in at day ten, handled by a nurse or MA with a standing protocol to escalate, accomplishes much of the same thing. The point is to close the distance between when something goes wrong and when you find out about it.
Perceived Cultural Alignment and Engagement
There’s a finding buried in the depression treatment literature that’s worth pulling forward. When patients with depression rate their providers on cultural competence, minority patients consistently report lower perceived cultural understanding than white patients, and those ratings track with engagement in care 3. The interesting part isn’t that the gap exists. It’s where the gap lives.
Perceived cultural alignment isn’t a function of whether you share a background with your patient. It’s a function of whether your patient feels like the version of themselves they brought into the room got taken seriously. That’s a different problem, and a more tractable one. You don’t need shared identity to communicate that you understood what someone told you. You need to ask follow-up questions that show you heard the specifics, not the category.
A practical example. A patient mentions that her mother thinks therapy is for white people and that she’s been quiet about starting an SSRI. The clinically lazy move is to validate generically and pivot to the symptom checklist. The move that builds alignment is to ask what her mother actually said, what she thinks about that, and whether the medication conversation at home is something she wants help thinking through. That takes ninety seconds. It changes whether she comes back.
The clinical competence framework that’s been proposed in the disparities literature names this directly: sociocultural awareness isn’t a separate domain from assessment and treatment planning, it’s integral to both, particularly for patients with serious mental illness 6. The patients who feel that integration are the ones who stay in care. The patients who don’t, don’t — and you see that downstream as a missed follow-up, a chart label that never gets revisited, or an adherence number that confirms a story about the patient instead of telling you something about the visit.
Four Decision Points to Audit in Your Next Ten Charts
If you want a low-friction way to put this article to work, pull your next ten charts from patients in racial or ethnic minority groups and run them through four questions. Not as a quality improvement project. As a thirty-minute self-audit between visits.
One: Did mood get a full hearing before psychosis became the organizing diagnosis? Look for documented PHQ-9, YMRS, or equivalent mood symptom data at intake. If the chart jumps from chief complaint to psychotic symptom inventory without a quantitative mood anchor, you’ve found a drift point. The Institute of Medicine review names systematic incorporation of sociocultural and longitudinal information into assessment as one of the clearest provider-level levers available 1.
Two: In patients carrying a schizophrenia or schizoaffective label, is there a mood stabilizer in the regimen, and if not, why not? Pull the longitudinal course. Episodic with interepisode functioning, family history of mood disorder, prior antidepressant-induced activation — these are the data points that should prompt a bipolar reconsideration and a mood stabilizer trial, not a fourth antipsychotic adjustment.
Three: For patients on an SSRI or SNRI, when was the first follow-up after initiation? If the default was four to six weeks across the board, you missed the window where most early discontinuations happen. A two-week touch — even a brief telehealth or nurse-led check — changes what you learn about side effects and what the patient learns about your continued involvement.
Four: For patients with poor adherence or premature discontinuation, what does the chart say about why? If the note reads “patient nonadherent” without specifics about side effects, beliefs, or fit with daily life, that’s a relational data gap, not a patient trait. The clinical competence framework treats sociocultural awareness as integral to assessment and treatment planning, not a separate domain 6. Adherence interpretation is one of the places that integration either happens or doesn’t.
Ten charts. Four questions. You won’t fix the literature with this. You’ll find your own drift points, which is the only place change actually starts.
If You Coordinate Referrals Across a Group Practice
A note for prescribers in group practices or multi-clinician settings who shape referral patterns for colleagues: the audit gets more useful when it moves up a level. The same drift points that show up in individual charts also show up in aggregate referral data, and you have visibility into both.
Look at where your group sends therapy referrals for patients with serious mental illness or complex mood presentations, and whether those referral patterns differ by patient demographics. If Black patients carrying psychotic disorder labels route reflexively to a narrow set of providers while white patients with similar acuity get a broader range of options, that’s a routing pattern worth surfacing in your next clinical meeting. The conceptual model of culturally responsive services treats the alignment between community characteristics and organizational practice as a quality variable, not a values question 14.
The other lever is intake documentation. If your group’s templates don’t prompt for quantitative mood scores, longitudinal episode history, or family psychiatric history at first visit, the drift documented in the diagnostic literature gets built into the workflow. Adjusting the template costs one meeting. It changes what every prescriber in the group sees on every chart.
Choosing a Therapy Referral Partner That Matches Your Standard
Most of what’s been covered so far sits inside your visit. The last piece sits outside it: who picks up the patient between your appointments. If you’re tightening your differential and your follow-up cadence, the therapy partner you refer to either reinforces that work or undoes it.
The criteria worth applying are narrower than the marketing language most practices use. First, ask whether the therapy team treats sociocultural context as part of assessment and treatment planning, or as a separate module bolted onto a standard intake. The clinical competence literature is direct about this distinction — cultural awareness is integral to assessment for patients with serious mental illness, not a parallel track 6. A practice that runs a generic intake and adds a cultural questionnaire at the end is doing something different than a practice that builds the cultural and longitudinal history into the formulation.
Second, ask how the therapy team communicates back to you. If a patient with a contested schizophrenia label is being reassessed through ongoing therapy contact, you want notes that flag mood episode history, family psychiatric data, and functional course — the information that would prompt a mood stabilizer trial. Therapy partners who treat the prescriber as part of an integrated care team produce better diagnostic clarity over time than those who operate in parallel 4.
At Mind Body Optimization, this is how the clinical model is built. We work across Texas, Tennessee, Oklahoma, and Missouri with prescribers who want therapy partners taking cultural responsiveness as seriously as they do — not as a training topic, but as part of the formulation. If that’s the kind of referral relationship you’re looking for, we’d welcome the conversation.
Schedule a session that centers your experience
Connect with clinicians who value your story and understand the impact of identity on mental health.
Frequently Asked Questions
How do I adjust my differential when a Black patient presents with both mood and psychotic features?
Build the mood differential first. Quantify mood symptom severity with a PHQ-9 or YMRS at intake, then ask whether the psychotic features fit as mood-congruent, mood-incongruent within an affective episode, or as a primary thought disorder. Reversing that sequence is where clinicians underweight depression in Black patients with comparable mood severity 9.
If adherence is a relational signal, what should I actually change in follow-up?
Pull the first follow-up after an SSRI start to two weeks instead of four to six. If a full visit isn’t feasible, a nurse-led phone or portal check at day ten with a standing escalation protocol catches side effects before they become reasons to stop. The Institute of Medicine review identifies follow-up cadence as a concrete provider-level lever 1.
What are the clinical implications of bipolar misdiagnosis for mood stabilizer prescribing?
Patients of African ancestry with bipolar disorder are more often misdiagnosed with schizophrenia and less likely to receive mood stabilizers 11. When psychotic features appear in a Black or Hispanic patient with a credible mood history, consider lithium, valproate, or lamotrigine alongside the antipsychotic question. Family history, prior antidepressant-induced activation, and episodic course should prompt a bipolar reconsideration before another antipsychotic adjustment.
How should I evaluate whether a therapy referral partner takes cultural responsiveness seriously?
Ask whether sociocultural context shapes their formulation or sits in a separate intake module. Clinical competence research treats cultural awareness as integral to assessment for serious mental illness, not a parallel track 6. Also ask how they communicate back to you on contested diagnoses — partners flagging mood episode history and functional course produce better diagnostic clarity over time than those operating in parallel 4.
Does racial concordance between prescriber and patient meaningfully change engagement?
The evidence points less to concordance itself and more to perceived cultural understanding. Minority patients with depression consistently rate providers lower on cultural competence, and those ratings track with engagement 3. You don’t need a shared background to communicate that you heard the specifics of what your patient told you. You need follow-up questions that engage the particulars, not the category.
What can I realistically audit in my own charts without adding hours to my week?
Pull ten recent charts from minority patients and check four things: quantitative mood data at intake, mood stabilizer presence in any schizophrenia or schizoaffective regimen, first follow-up timing after SSRI initiation, and specificity in adherence documentation. Thirty minutes between visits surfaces your own drift points. Systematic incorporation of sociocultural and longitudinal information into assessment is a documented provider-level lever 1.
References
- Racial and Ethnic Disparities in Diagnosis and Treatment for Mental Health Conditions. https://www.ncbi.nlm.nih.gov/books/NBK220337/
- Exploring racial and ethnic disparities in medication adherence among older adults receiving medication therapy management services. https://pmc.ncbi.nlm.nih.gov/articles/PMC9009823/
- Racial and Ethnic Differences in Patients’ Perception of Providers’ Cultural Competence in Depressive Disorder Treatment. https://pmc.ncbi.nlm.nih.gov/articles/PMC10688309/
- Toward Culturally Centered Integrative Care for Addressing Mental Health Disparities Among Ethnic Minorities. https://pmc.ncbi.nlm.nih.gov/articles/PMC4228792/
- A Cultural Competence Approach to Improving Mental Health of Racial/Ethnic Minority Groups. https://dbh.ohio.gov/wps/portal/gov/dbh/community-partners/advisory-groups/documents/reconceputalizing-access
- Addressing Mental Health Disparities Through Clinical Competence. https://pmc.ncbi.nlm.nih.gov/articles/PMC2659411/
- Reframing Culturally Competent Care to Improve Mental Health Outcomes for Minority Populations. https://repository.usfca.edu/cgi/viewcontent.cgi?article=2737&context=capstone
- Racial disparities in psychotic disorder diagnosis: A review of empirical literature. https://pmc.ncbi.nlm.nih.gov/articles/PMC4274585/
- African Americans More Likely to Be Misdiagnosed with Schizophrenia, Rutgers Study Finds. https://www.rutgers.edu/news/african-americans-more-likely-be-misdiagnosed-schizophrenia-rutgers-study-finds
- Racial and Ethnic Disparities in Mental Health Care. https://pmc.ncbi.nlm.nih.gov/articles/PMC3928067/
- Racial disparities in bipolar disorder treatment and research: A call to action. https://pmc.ncbi.nlm.nih.gov/articles/PMC6175457/
- Racial Differences in Adherence to Antidepressant Treatment in Medicaid-Enrolled Patients with Major Depressive Disorder. https://pmc.ncbi.nlm.nih.gov/articles/PMC3573214/
- Ethnic disparities in medication adherence? A systematic review of the literature. https://pmc.ncbi.nlm.nih.gov/articles/PMC9946219/
- A Literature Review and Conceptual Model for Mental Health Services. http://cfs.cbcs.usf.edu/projects-research/_docs/CC_PsychService_2009.pdf